Pneumonia Detection with Deep Learning
MPHY 6120 · Homework 5 · PneumoniaMNIST Results
4708
Training Images
624
Test Images
0.970
Best AUC
1
Missed Pneumonia (FN)
Part 1: Data Exploration
PneumoniaMNIST: 1214 normal, 3494 pneumonia in training set. The dataset is imbalanced (~75% pneumonia), which means accuracy alone is misleading.
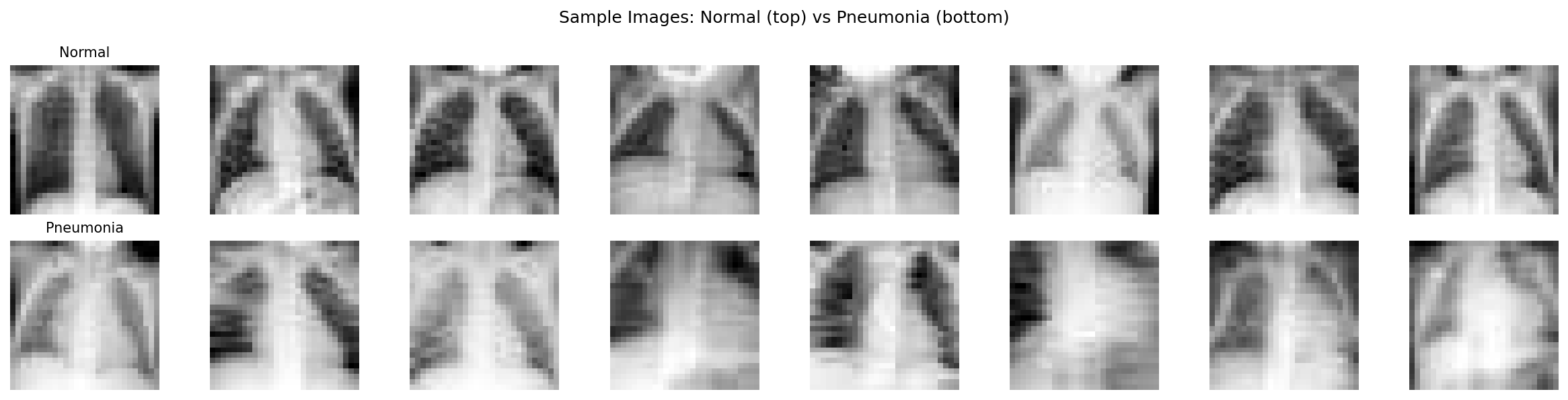
Normal chest X-rays (top) vs pneumonia (bottom). Even at 28×28 resolution,
pneumonia cases show increased opacity in the lung fields.
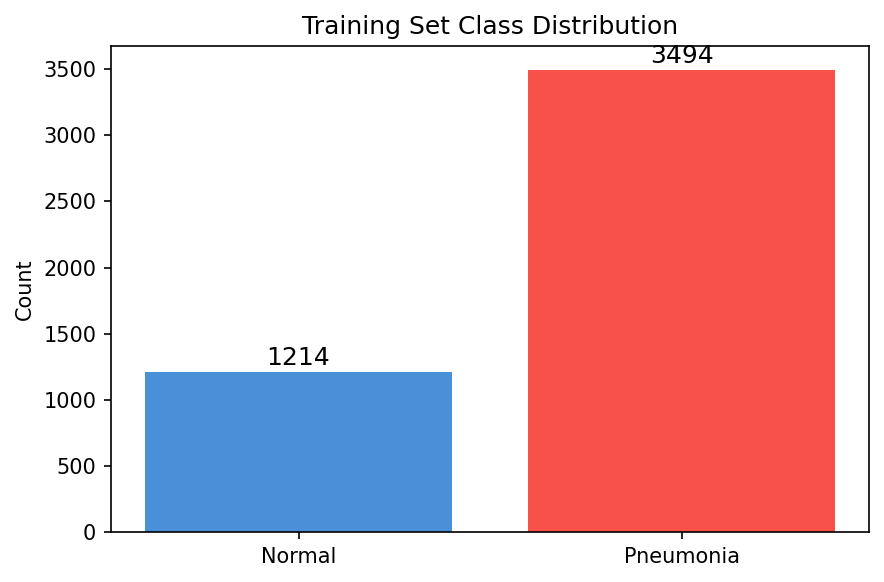
Training set class distribution — significant imbalance toward pneumonia.
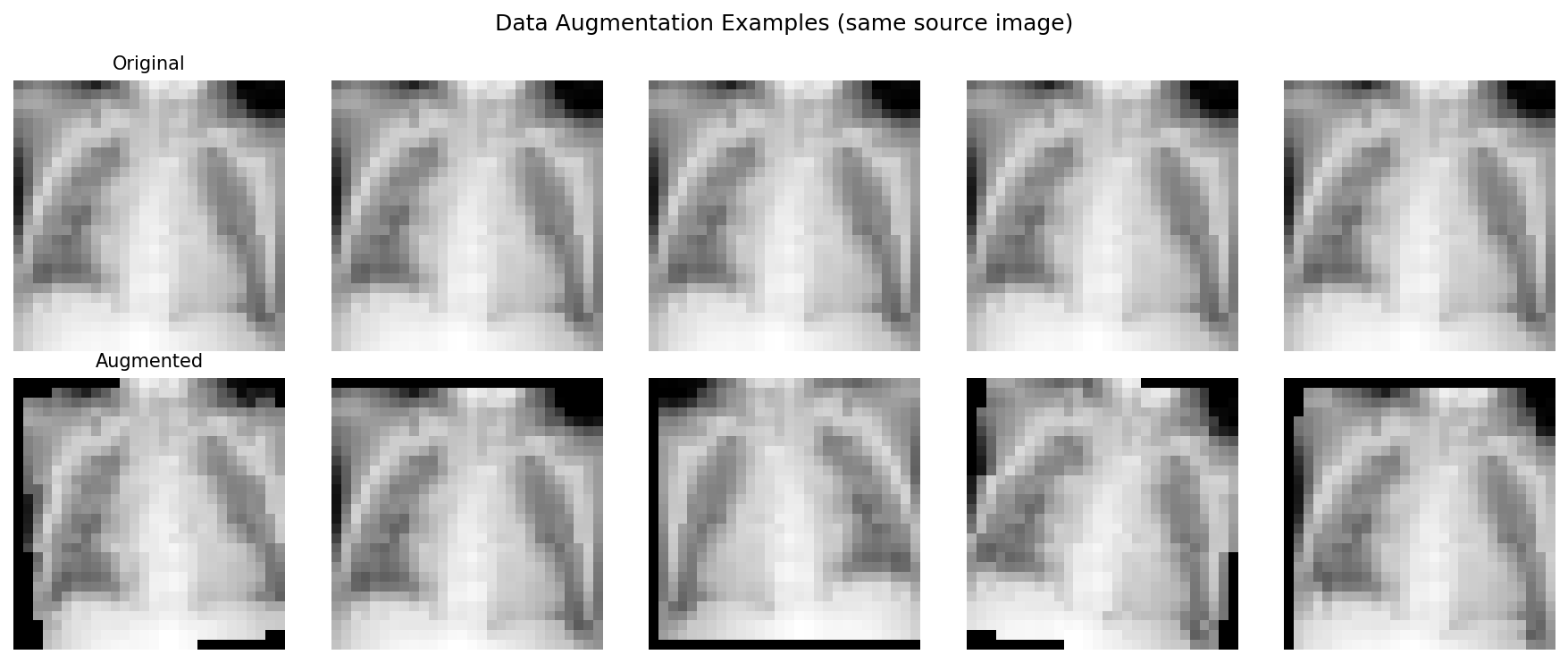
Data augmentation creates training variety through flips, rotations,
translations, and brightness changes — all clinically safe transformations.
Part 2: Simple CNN
3-layer CNN with BatchNorm and dropout: 93,249 parameters. Architecture: Conv(32) → Conv(64) → Conv(128) → AdaptiveAvgPool → FC(1).
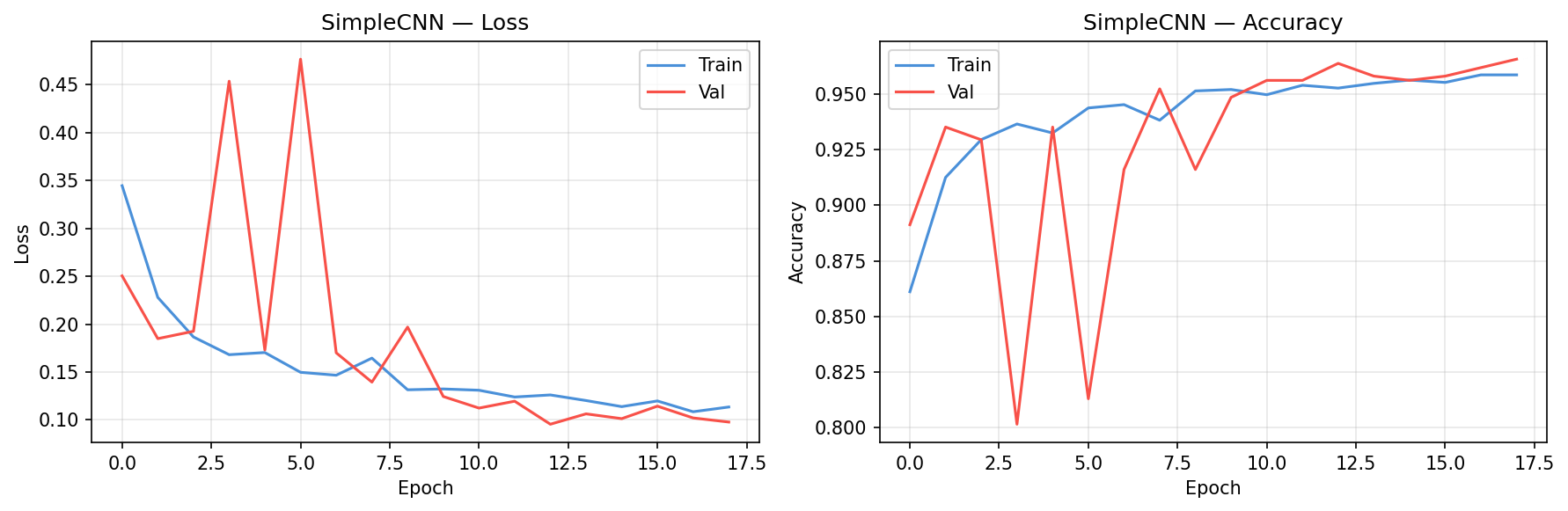
SimpleCNN training curves showing loss and accuracy convergence.
Part 3: Transfer Learning
Key insight: Transfer learning with pretrained ResNet18 outperforms training from scratch,
even though ImageNet contains no medical images. Low-level visual features (edges, textures) are universal.
.png)
ResNet18 (pretrained) training curves — two-stage fine-tuning with frozen backbone
followed by full model training at lower learning rate.
Model Comparison
| Model | Accuracy | AUC | Precision | Recall | F1 |
|---|---|---|---|---|---|
| SimpleCNN | 0.851 | 0.955 | 0.815 | 0.985 | 0.892 |
| ResNet18 (scratch) | 0.859 | 0.969 | 0.819 | 0.995 | 0.898 |
| ResNet18 (pretrained) | 0.888 | 0.970 | 0.849 | 0.997 | 0.917 |
Part 4: Evaluation
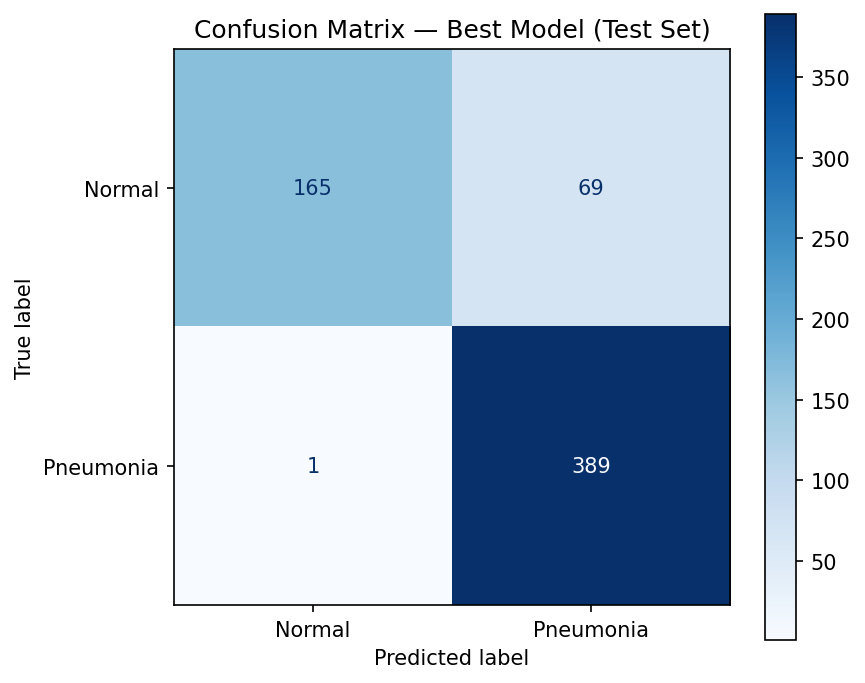
Confusion matrix on the test set. Focus on false negatives (bottom-left) —
these are missed pneumonia cases.
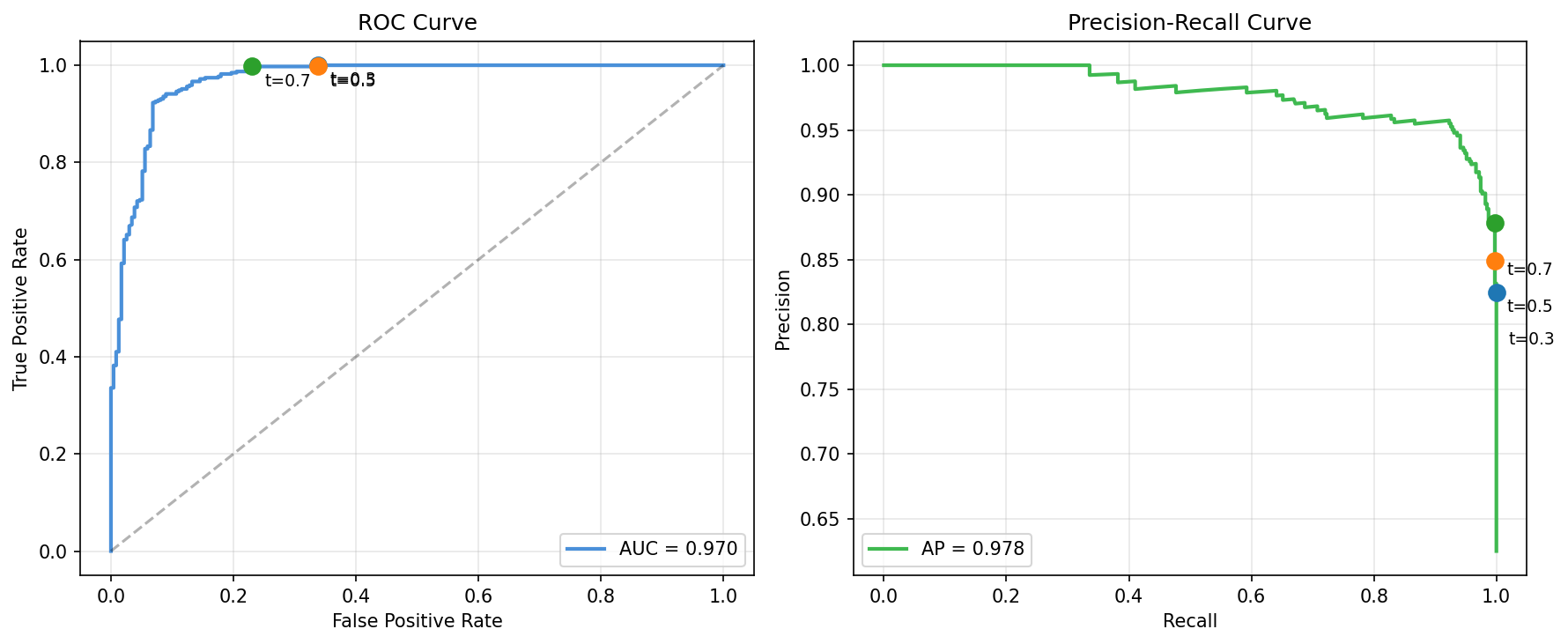
ROC curve (left) and Precision-Recall curve (right) with operating points
at different thresholds. For pneumonia screening, we'd choose a low threshold to maximize recall.
Clinical reality: A model with AUC=0.970 on 28×28 images
is a proof of concept, not a deployable system. Real pneumonia detection requires full-resolution images,
multi-label classification, and validation across institutions.
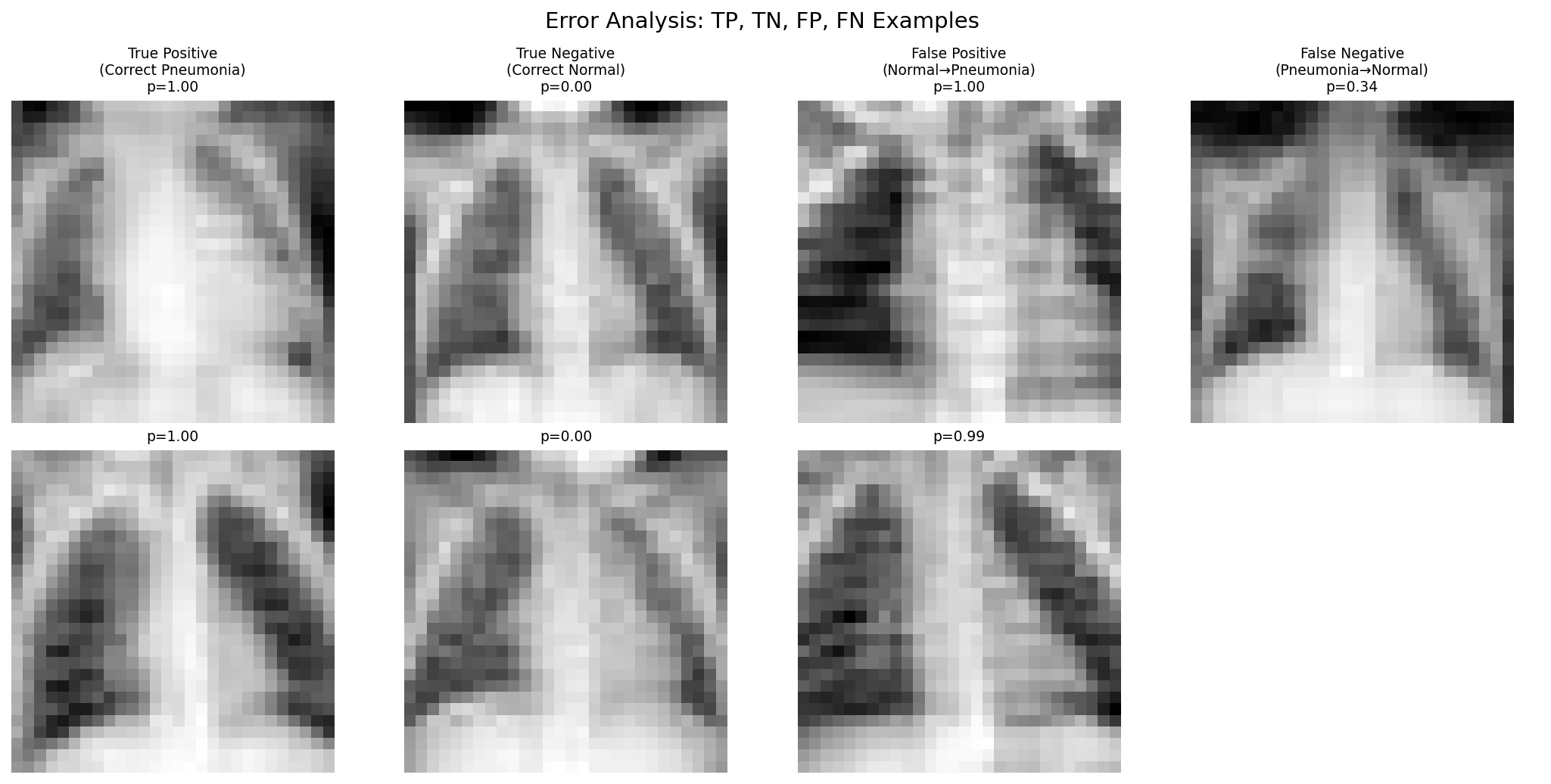
Error analysis: true positives, true negatives, false positives, and false negatives.
False negatives tend to be subtle cases; false positives often have prominent vascular markings.
Part 5: Interpretability
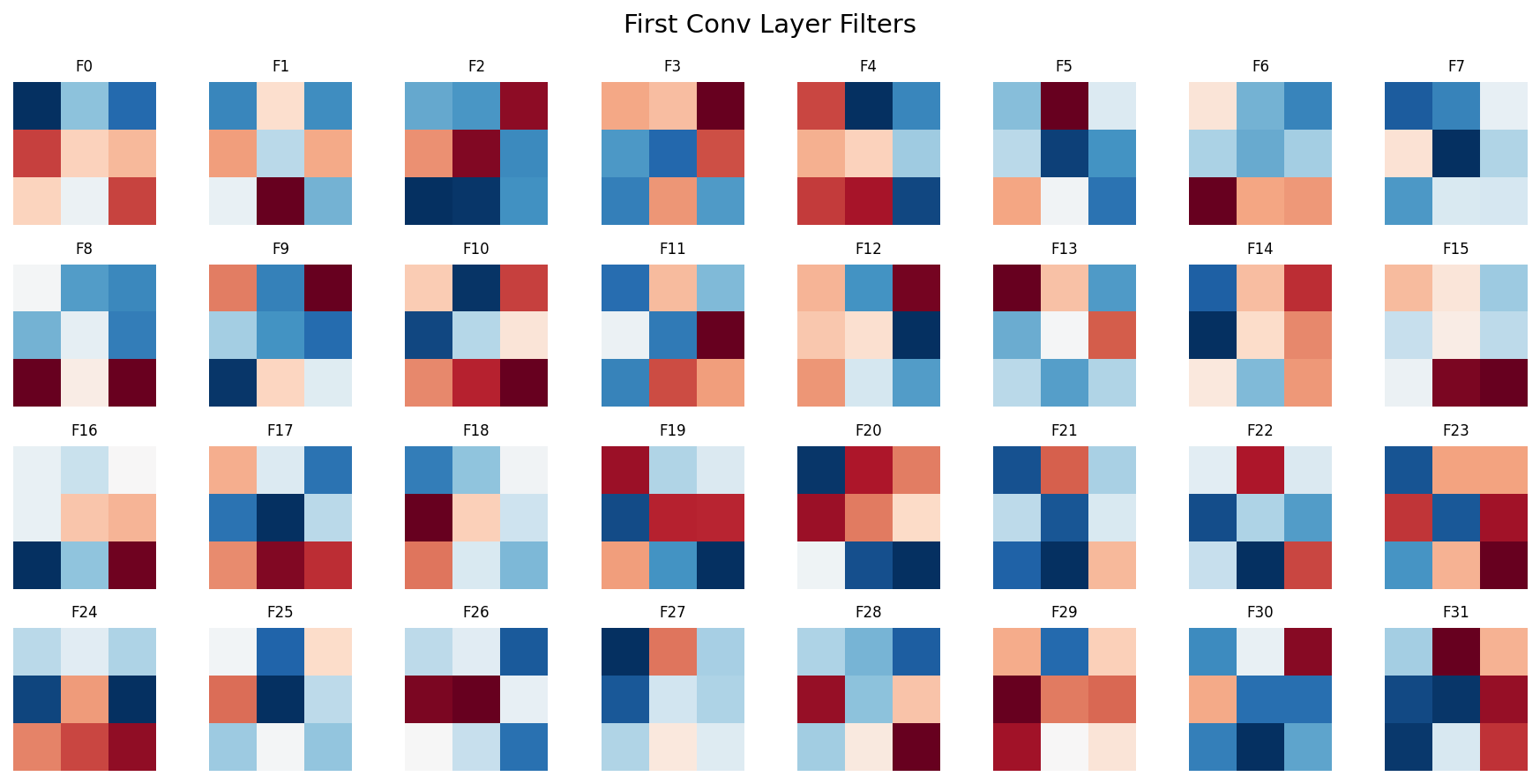
Learned filters from the first convolutional layer — detecting edges,
gradients, and simple textures that form the basis of higher-level feature detection.
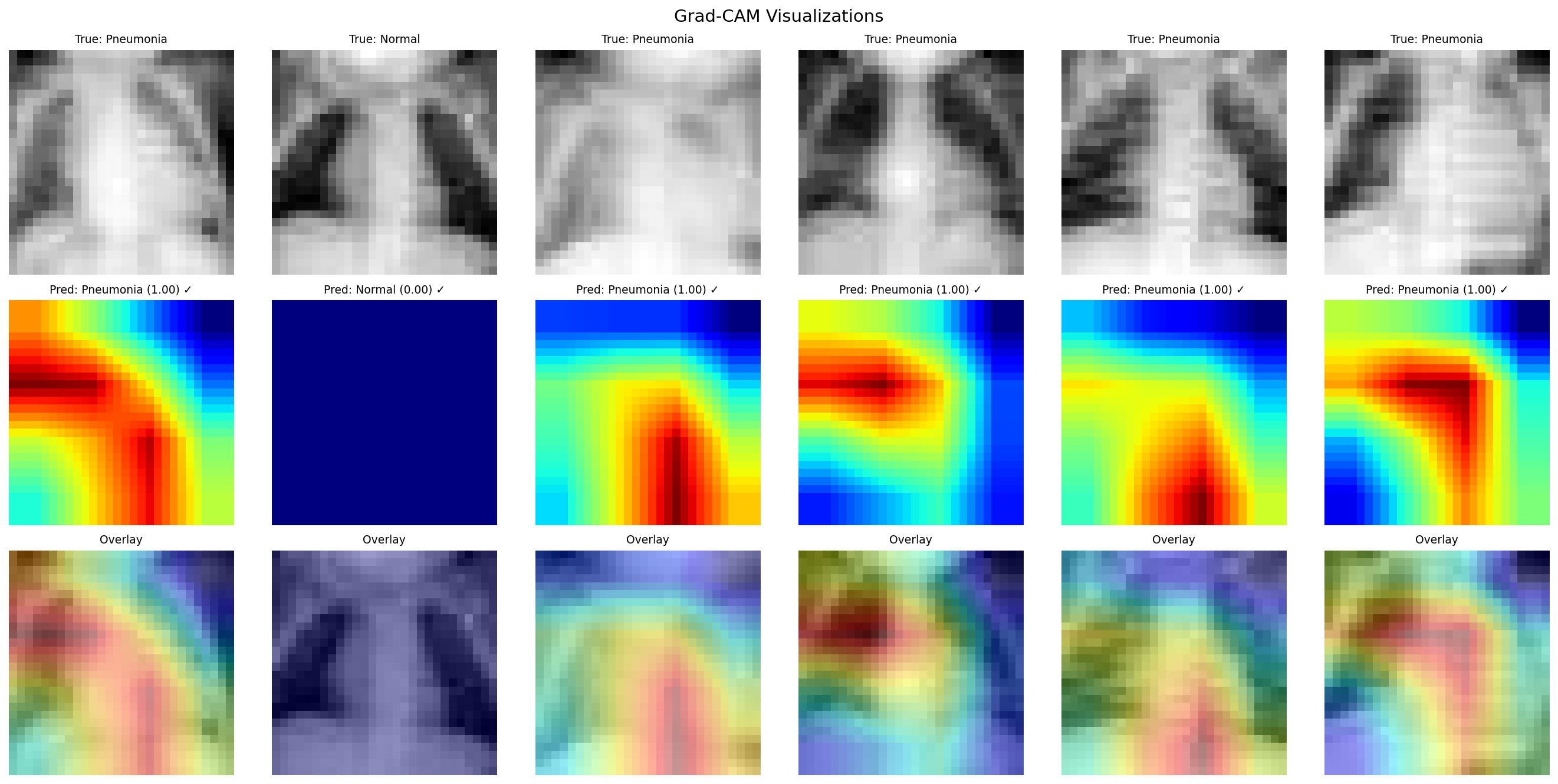
Grad-CAM visualizations showing where the model focuses. Top: original images.
Middle: activation heatmaps. Bottom: overlay. The model attends to lung fields and areas of opacity.
What we learned: A pretrained ResNet18, fine-tuned with augmentation, achieves strong
performance on pneumonia detection even at 28×28 resolution. Transfer learning consistently
outperforms training from scratch on small medical datasets. But AUC alone doesn't tell the clinical
story — per-class recall and error analysis are essential for understanding real-world impact.